
The SI joint. What the heck is up with the SI joint?

SI stands for sacroiliac, which describes the joint between the sacrum (lower part of your spine) and the ileum (one of the bones that makes up the pelvis). The SI joint is an interesting one for me, mainly due to many healthcare providers eliciting fear surrounding it. What do I mean by that? Well, have you heard someone say their SI joint is “out of place?” I have. Too many times.
Peter O’Sullivan, a leading clinician, researcher, and educator of musculoskeletal pain disorders talks about how clinical labels of the pelvis being “displaced” or “unstable” can be “detrimental with the potential to render the patient passively dependent on someone to ‘fix them,’ elevating anxiety levels, reinforcing avoidance behaviors and promoting disability.”
Well said, in my opinion.
Let’s decode this. When patients hear “your SI joint is out of place,” it tends to make them feel reliant on someone to “fix them” and makes them fear movements and activities that will put their SI “back out of place,” creating completely unnecessary fear.

The SI joint actually has less than 4 degrees of rotational movement and less than 1.6mm of translatory movement. Layman’s terms? Your SI can NOT go out of place unless there is significant trauma or potentially milder trauma in the case of an individual with a connective tissue disorder. This is GREAT news! It means that your SI joint is, in fact, in place.
Okay, but Doctor Kate, I swear it feels like my SI joint is out.
YES! I believe you! The SI joint is surrounded by a lot of innervated tissues, which is why people feel like it’s out of place even though it hardly moves! But, if someone tells you they can feel your SI joint is out of place, I would be a little suspicious. It’s been found that movement of the SI joint can NOT be reliably assessed by palpation (someone feeling your pelvis with their hands). Plus, if there are observable asymmetries, they are likely secondary to changes in muscle activity NOT in the position of the joints themselves.
NO study using a valid measurement tool has shown that manipulations alter the position of the pelvic joints. The relief you get after a manipulation is likely the result of pain inhibition from your brain and spinal cord secondary to the quick stretch of your joint or as the result of a change in activity of the muscles around the pelvis. So, what can you do to make it feel like it’s in place without having to repeatedly get an adjustment? I may be biased, but I recommend a physical therapist.

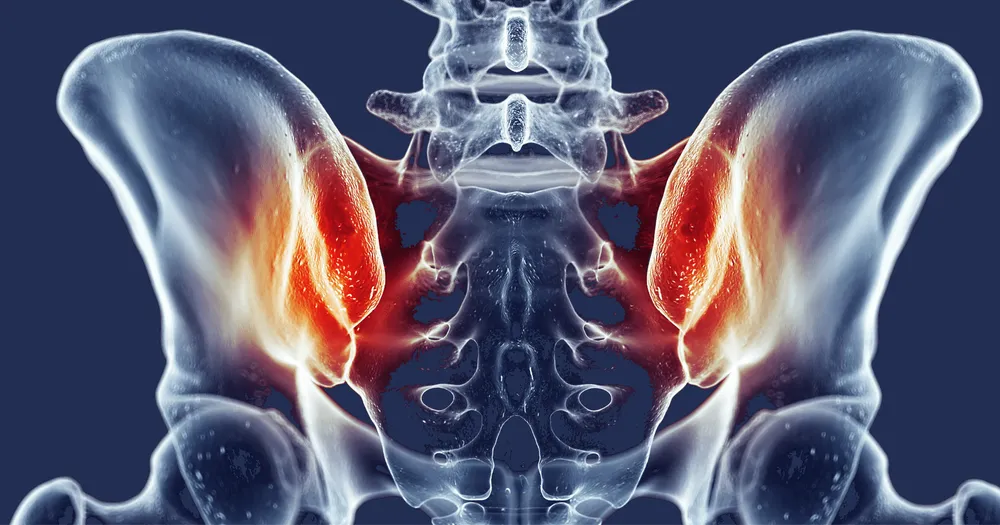
Pelvic Girdle Pain locations
Let’s talk about the classifications of pelvic girdle pain (aka SI joint pain). Pelvic girdle pain is most commonly associated with either excessive or insufficient muscle activation of the lumbopelvic and surrounding musculature. In the physical therapy world, these two categories are called “Reduced Force Closure” and “Excessive Force Closure.”
Reduced force closure means that there is excessive strain on the SI joint and/or its surrounding connective tissue due to a lack of muscle strength/control. This classification is common with more flexible individuals. Due to a lack of strength in the muscles around the pelvis, the load going through the area is less than ideal, leading to higher stress in some areas versus others, resulting in pain.
Those with pain related to reduced force closure get short-term relief from mobilization, massage, and other manual techniques. The emphasis here is short-term. While it may provide temporary relief, it won’t solve the pain. On the other hand, training the muscles around the pelvis that support strength and stability will improve symptoms long term.
The other category is excessive force closure. The funny thing about this group is that they often think they need MORE pelvic stability and are overtraining the muscles around their pelvis. Yes, there is such a thing as too much strength training. Abnormal and sustained loading of the tissues around the pelvis in this classification cause pain.
It’s common for those in this group to think that their pelvis is “unstable” or “displaced.” This leads to higher levels of strength training resulting in more discomfort, in turn triggering fear about the “stability” of their pelvis. Cue more worrying and overtraining, which creates a vicious cycle. Did that sentence make you anxious or what? We feel you. Typically, those in the excessive force closure category have higher levels of stress and anxiety. Pain relief comes from general cardiovascular exercise, stretching, and massage. Management for this group involves reducing “force closure” aka muscle activation across the pelvis. Interventions include relaxation strategies, breathing exercises, muscle inhibitory techniques, cessation of stabilization exercises, and a focus on cardiovascular exercises.

The DPTs at MOTION RX are able to both identify and treat SI joint related pain.
During your initial evaluation, your physical therapist should take a detailed history, including onset of symptoms, aggravating factors, and easing factors related to the pain. From there, the therapist should already have a hypothesis of what may be going on. Your PT should then do a physical examination in which they establish the involvement or lack thereof in the lumbar spine, hip, and SI joint. Based on the physical examination, your therapist should know which category of SI related pain you fall into and will dose exercises appropriately.